Chapter 1
Lesson Objectives By the end of this lesson, fosters will: Understand why we track what we track. Know how to use the medical and daily logs
Recognize red flags that require escalation
Feel empowered (not afraid) to report concerns
Core rationale
If it isn’t written down, it didn’t happen.
Medical patterns are invisible without logs.
Accurate paperwork protects:
the animal
the foster
the rescue
the veterinarian
Core Philosophy
Observation beats assumption
Patterns matter more than moments
Early reporting prevents emergencies
Paperwork is part of fostering. Click the link for the log featured in this lesson. Be sure to open in a new tab.
https://docs.google.com/spreadsheets/d/1PNySqwtd9R2YRO5OzkI2U8uv1uqR4KLogkWSRDCClm8/edit?usp=sharing
Lesson Outline
1. Why We Track
Weight trends matter more than single numbers
Appetite changes often precede illness
Stool changes are one of the earliest warning signs
Vets diagnose patterns, not vibes
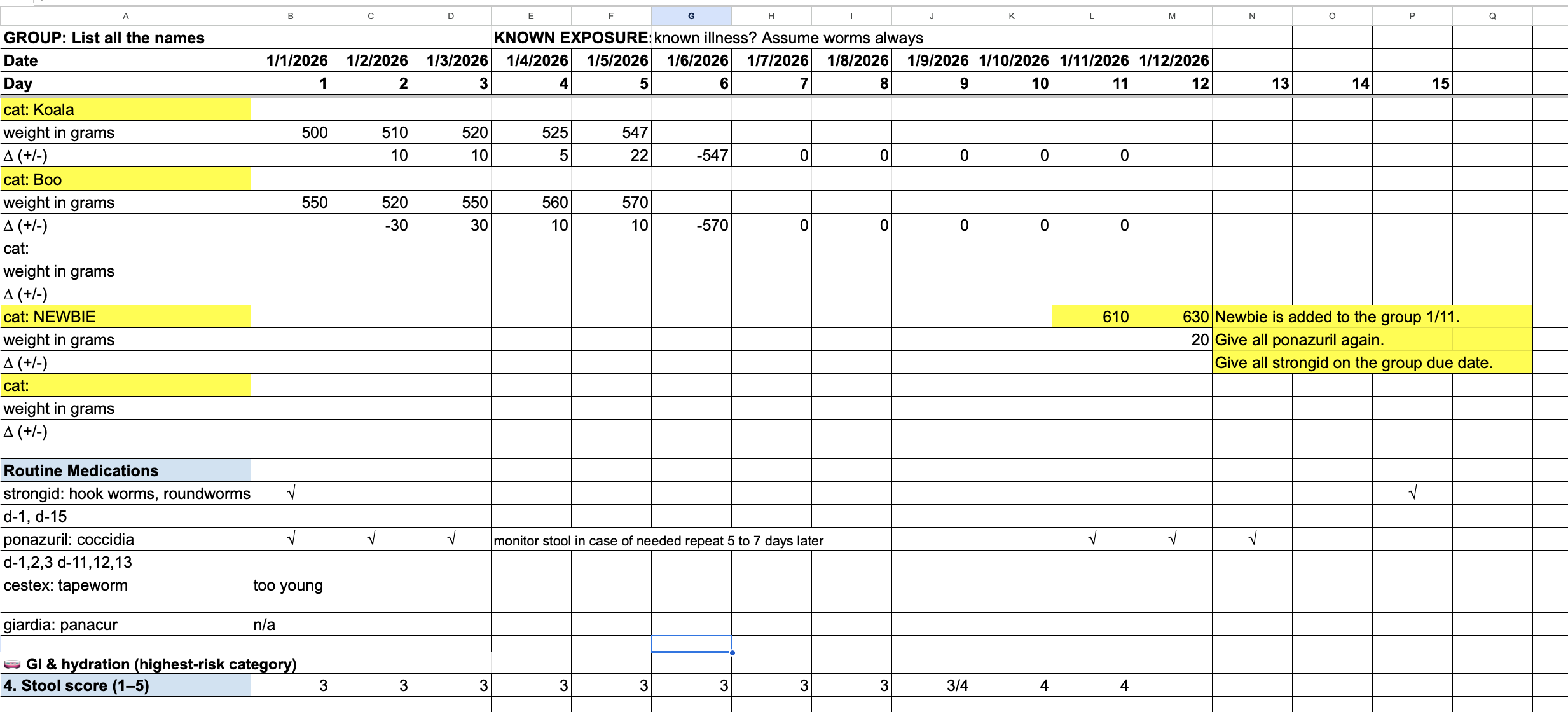
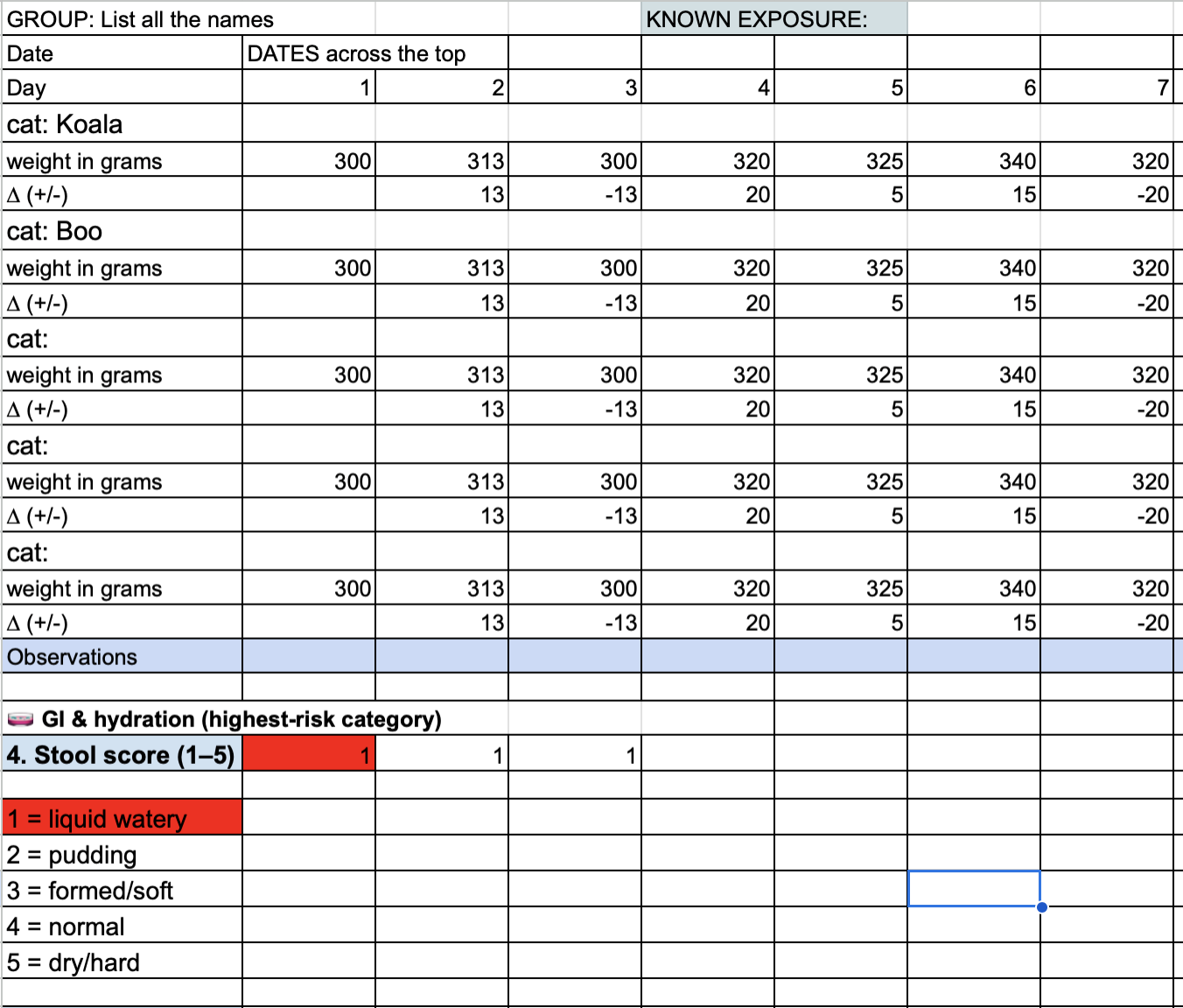
2. How to Use the Logs
Daily weight tracking
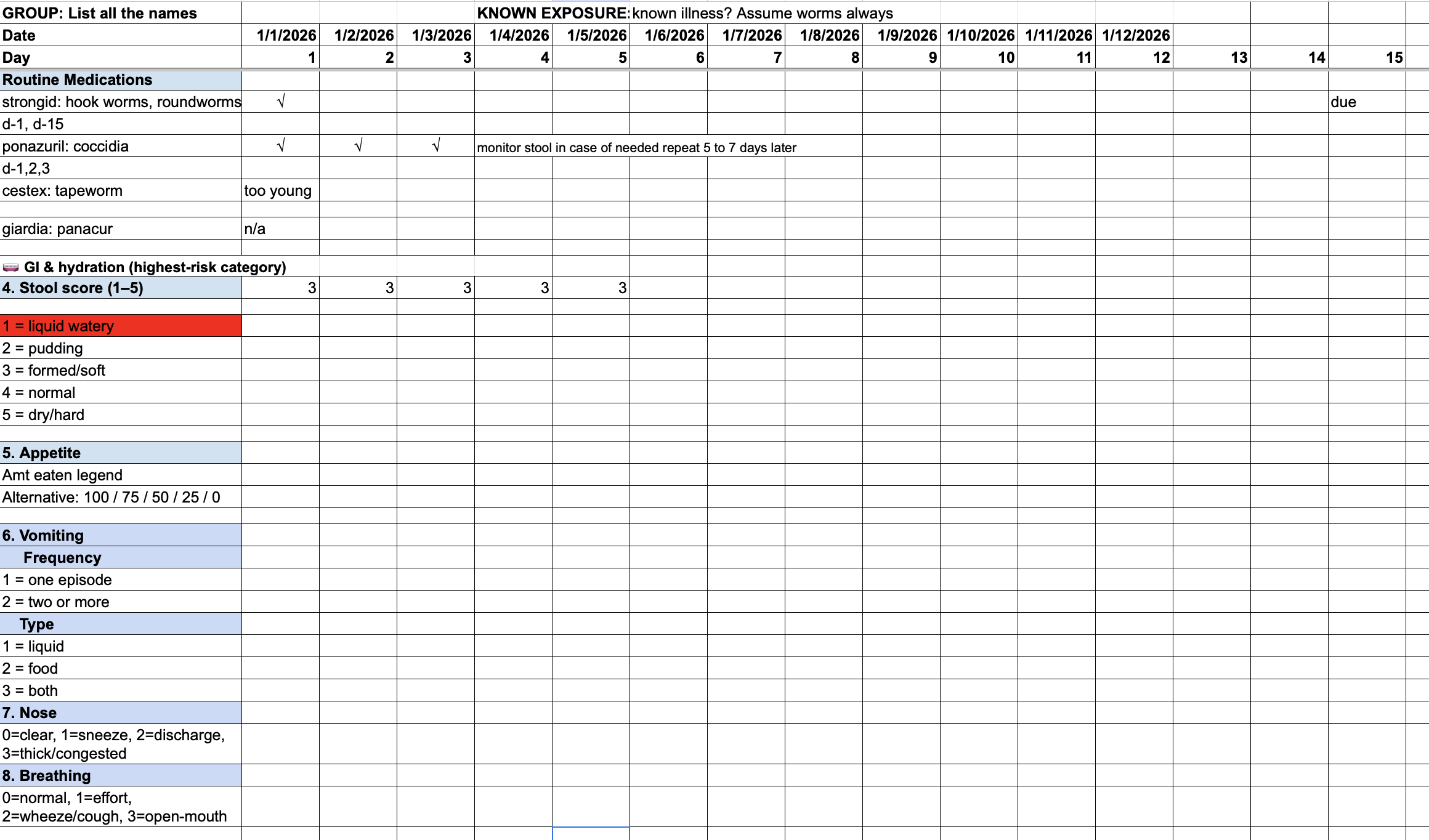
Stool consistency tracking (numeric scale)
Appetite tracking (what + how much)
Notes on behavior, energy, hydration, and symptoms
Short notes are fine
Consistency matters more than perfect wording
One line per day is enough if done daily
Key:
“You don’t need to diagnose — just observe and record.”
3. Thresholds for Escalation
Clear, concrete triggers for contacting the rescue team:
Escalate if:
Weight loss or plateau in young kittens
Diarrhea lasting more than 24 hours
Lethargy, hiding, or sudden behavior change
Not eating or eating significantly less
Vomiting
Any ‘something feels off’ instinct
4. Permission Statement
This is critical for new fosters.
You are not expected to know everything
Asking questions is a strength
Early reporting saves lives
Silence is the only mistake
Rolling Intake Medication Synchronization Decision Tree
For Co-Housed Foster Animals
START
A foster brings a new animal into a home with existing foster animals.
STEP 1: Are there animals already in the home?
☐ NO
→ Treat new intake per standard intake protocol
→ Assign Day 0 for that animal
→ End
☑ YES
→ Go to Step 2
STEP 2: Are animals co-housed or sharing resources?
(litter boxes, bowls, airspace, hands, surfaces)
☐ NO (fully separated)
→ Treat new intake independently
→ No synchronization required
→ End
☑ YES
→ Go to Step 3
STEP 3: Are the existing animals currently on an intake medication schedule?
☐ NO
→ Go to Step 4
☑ YES
→ Go to Step 5
STEP 4: Existing Animals NOT on Intake Meds
Assumption:
Shared space = shared exposure.
Action:
All animals (existing + new) start intake meds together
Assign one shared Day 0
Use one unified schedule
Track animals individually, treat as a group
📌 Key rule:
Do not stagger intake meds in shared housing.
→ End
STEP 5: Existing Animals ARE on Intake Meds
5A. Are they in the active treatment window?
(before any post-treatment countdown begins)
☑ YES
New intake joins immediately
Receives intake meds the same day
Schedule continues uninterrupted
No clock reset
📌 Key rule:
New intake joins the train. The train does not stop.
→ End
5B. Are they in the post-treatment waiting / observation period?
☑ YES
→ Go to Step 6
STEP 6: Post-Treatment Period + New Intake
At this stage, co-housing breaks containment.
Required action:
Reset the intake schedule
All animals (existing + new) return to intake meds
Assign a new Day 0 for the entire group
Start countdown the day after the new treatment
📌 Key rule:
You cannot preserve a clean window once a new untreated animal enters shared space.
→ End
STEP 7: Special Situations
Different ages / weights
Dose individually
Schedule stays unified
One animal symptomatic, others not
Treat all exposed animals
Symptoms drive urgency, not membership
“Temporary” co-housing
(overnight, playtime, shared supplies)
Considered exposure
Follow the same tree
Partial separation
(crate rotation, baby gates, shared air)
Considered shared exposure
Follow the same tree
NON-NEGOTIABLE PRINCIPLES
Shared space = shared schedule
Intake meds are group-based
Rolling intake resets clocks
Staggering causes failure loops
This is a system decision, not a foster judgment
What This Prevents
Endless retreatment
‘Mystery’ reinfections
Foster frustration
Medical burnout
Blame cycles
Coccidia Treatment Synchronization Decision Tree
Rolling Intake – Shared Foster Space
START
A foster brings a new kitten into a home with existing foster kittens.
STEP 1: Are there kittens already in the home?
☐ NO
→ Treat new kitten per standard intake protocol
→ Start Day 0 for that kitten
→ End
☑ YES
→ Go to Step 2
STEP 2: Are the existing kittens currently on a coccidia treatment schedule?
☐ NO (not currently being treated)
→ Go to Step 3
☑ YES (mid-treatment or between rounds)
→ Go to Step 4
STEP 3: Existing kittens NOT currently on treatment
Assumption:
Exposure is already shared the moment kittens co-house.
Action:
All kittens (new + existing) start treatment together
Designate the same Day 0 for everyone
Use one shared treatment calendar
📌 Key rule:
You do not treat the new kitten separately.
Logging:
Note “rolling intake – synchronized start”
Track weights individually, treatment collectively
→ End
STEP 4: Existing kittens ARE currently on treatment
This is the most common failure point — so this step is strict.
4A. Is the existing group within the first treatment window?
(early phase, before the post-treatment countdown begins)
☑ YES
Add the new kitten immediately
New kitten receives treatment same day
All kittens remain on the same schedule
No clock reset
📌 Key rule:
New kitten joins the train — the train does not stop.
→ End
4B. Is the existing group already in the post-treatment waiting period?
(countdown days already started)
☑ YES
→ Go to Step 5
STEP 5: Post-Treatment Countdown + New Intake
At this point, shared space = shared exposure.
Required action:
Reset the schedule
All kittens (existing + new) are placed back on treatment
A new Day 0 is assigned for the entire group
📌 Key rule:
You cannot “protect” treated kittens once a new untreated kitten is added.
Logging:
Note “reset due to rolling intake”
Start new countdown the day after the new treatment
→ End
STEP 6: Special Situations
Different ages / weights
Dose individually
Schedule remains unified
One kitten symptomatic, others not
Treat all exposed kittens
Symptoms determine urgency, not membership
Single kitten added briefly (“just overnight”)
Still considered exposure
Follow same decision tree
NON-NEGOTIABLE PRINCIPLES
Coccidia management is group-based, not individual
Shared litter = shared organism
Rolling intake resets clocks
Desynchronization causes reinfection loops
This is a systems issue, not a foster failure
(Important)
“If kittens share space, they share parasites — so they share a schedule.”
What This Prevents
Endless retreatment
“Why won’t this clear?”
Foster frustration
Blame spirals
Medical burnout